 Image of alcoholic beverages.[5]
Image of alcoholic beverages.[5]
Alcohol is a liver toxin that causes damage to the liver after prolonged consumption of the substance. Alcoholic liver disease is usually a result of alcohol toxicity. Alcoholic liver disease (ALD) causes approximately 20,000 deaths per year in the UK and is caused by heavy alcohol consumption. It is a major cause of malaise and mortality. Individuals vary in their susceptibility to ALD, however, advanced forms of alcoholic liver disease which include; steatohepatitis, cirrhosis and fibrosis could develop in individuals that consume large amounts of alcohol on a regular basis. [1] Other forms of ALD include steatosis. [2]
Steatosis and oxidative stress are the main metabolic consequences of prolonged alcohol consumption. The metabolism of alcohol changes the intracellular redox state. Its metabolism involves ethanol being oxidized by cytosolic alcohol dehydrogenases to acetaldehyde and mitochondrial aldehyde dehydrogenases oxidizing it into acetate. These reactions involve the reduction of NAD to NADH which affects the metabolism of carbohydrates and lipids. Substrates required in the citric acid cycle are diminished due to the impairment of gluconeogenesis causing acetyl coA to be redirected towards fatty acid synthesis and ketogenesis.[1] This altered redox state leads to the prevention of mitochondrial fatty acid β-oxidation which in turn leads to the development of steatosis (fatty liver), the early stage of ALD.[1] The up-regulation of sterol regulatory element-binding protein 1c (SREBP-1c) by ethanol increases the production of fatty acids in hepatocytes. SREBP-1c is a transcription factor that is involved in promoting fatty acid synthesis through the up-regulation of lipogenic genes.[3]
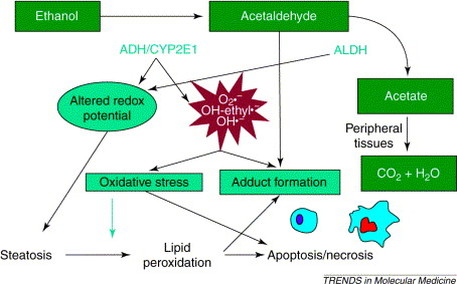
Illustration showing reactions that occur in the metabolic breakdown of alcohol[1]
Ethanol inhibits AMPK which plays a crucial role in fat metabolism. AMPK is a serine-threonine kinase that phosphorylates and inactivates enzymes that take part in fatty acid synthesis and fatty acid oxidation. AMPK also inhibits SREBP activity in hepatocytes by directly phosphorylating SREBP and thus attenuating steatosis. Through this AMPK can promote fatty acid oxidation while preventing fatty acid synthesis.[3]
Alcoholic hepatitis consists of hepatocyte injury, pericellular fibrosis and neutrophil infiltrate. Hepatocyte injury in alcoholic hepatitis is thought to be brought about by three mechanisms:
Chronic liver injury leads to a wound-healing response known as liver fibrosis.[3] The hallmark of alcoholic liver fibrosis is the deposition of collagen enveloping hepatocytes and is distributed in the perisinusoidal space. Alcoholic liver fibrosis can then progress to micronodular cirrhosis which can eventually become macronodular following abstinence from alcohol. Fibrosis brought about by alcohol is thought to be a healing response in regards to the preceding alcoholic hepatitis; cytokines released during hepatic injury activate fibrosis-producing hepatic stellate cells. Studies suggest that lipid peroxidation products and acetaldehyde may activate hepatic stellate cells which leads to the fibrogenic effect of alcohol.[3]
Alcoholic hepatitis consists of hepatocyte injury, pericellular fibrosis and neutrophil infiltrate. Hepatocyte injury in alcoholic hepatitis is thought to be brought about by three mechanisms:
- Oxidative stress during alcohol metabolism leading to peroxidative damage to the hepatocytes’ membrane phospholipids. The damage done to mitochondrial membranes leads to the irreparable necrosis and apoptosis.
- Hepatocyte apoptosis and oxidative stress can also be contributed to the release of tumour necrosis factor α (TNFα) through endotoxins.
- The binding of lipid peroxidation products and acetaldehyde to proteins leads to immunological processes against neo-antigens leading to the formation of adducts.[4]
Chronic liver injury leads to a wound-healing response known as liver fibrosis.[3] The hallmark of alcoholic liver fibrosis is the deposition of collagen enveloping hepatocytes and is distributed in the perisinusoidal space. Alcoholic liver fibrosis can then progress to micronodular cirrhosis which can eventually become macronodular following abstinence from alcohol. Fibrosis brought about by alcohol is thought to be a healing response in regards to the preceding alcoholic hepatitis; cytokines released during hepatic injury activate fibrosis-producing hepatic stellate cells. Studies suggest that lipid peroxidation products and acetaldehyde may activate hepatic stellate cells which leads to the fibrogenic effect of alcohol.[3]
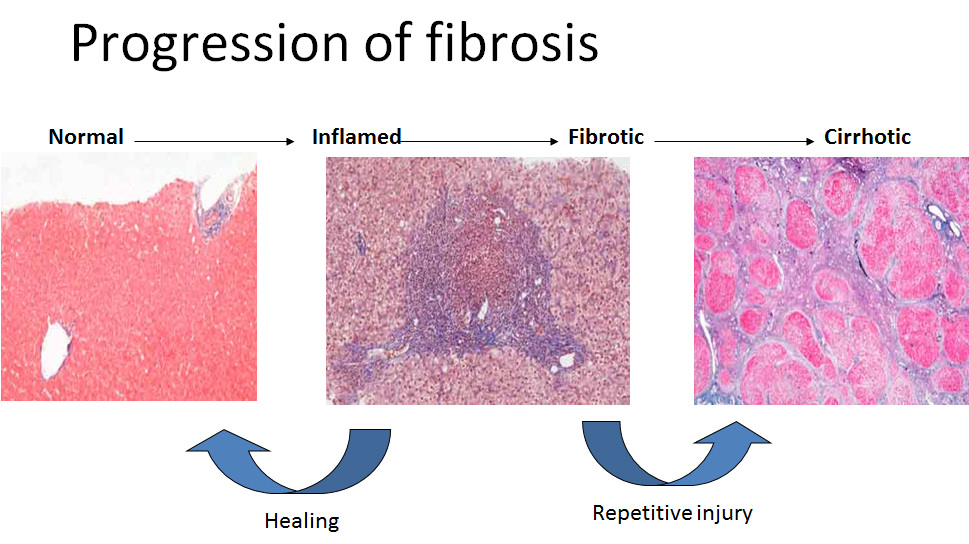
Illustration showing progression of liver fibrosis and cirrhosis.[6]
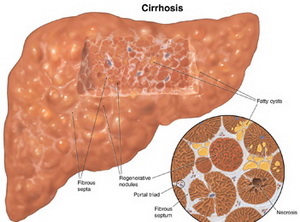
Image of cirrhotic liver.[7]
Increased studies on oxidative stress and hepatocyte injury has significantly increased the understanding of the pathogenesis of alcoholic liver disease. However, there are no FDA-approved treatments for the disease but certain pharmacotherapies targeting the main mechanisms of cell injury, along with abstinence from alcohol, are the current treatment strategies being used. Abstaining from alcohol use can increase resolution of steatosis and can improve survival in patients with cirrhosis, even though they might have decompensated liver function. Glucocorticosteroids are used in the treatment of alcoholic hepatitis because they inhibit pro-inflammatory transcription factors which include nuclear factor-κB (NF-κB) and activator protein 1 (AP-1), and they have significant effects on pro-/anti-inflammatory cytokine levels; all mechanisms of action which are beneficial in treating patients with alcoholic hepatitis. Antioxidants are being studied in treating ALD in order to diminish oxidative stress associated with the disease. Unfortunately, the use of antioxidants in clinical trials has been disappointing.[8]
|
Video showing liver cirrhosis caused by alcohol.[9]
|
Barbara Amolo. Last updated: March, 2015
|
References
- Stewart, S., Jones, D. and Day, C.P. (2001) “Alcoholic liver disease: new insights into mechanisms and preventative strategies” Trends in Molecular Medicine, 7(9):408-413.
- Diehl, A.M. (2002) “Liver disease in alcohol abusers: clinical perspective.” Alcohol, 27(1):7-11.
- Gao, B. and Bataller, R. (2011) “Alcoholic Liver Disease: Pathogenesis and New Therapeutic Targets” Gastroenterology, 141:1572-1585.
- Day, C.P. (2002) “Alcohol and the Liver” Medicine, 30(11):18-20.
- Leyva, J. (2013) “Does Alcohol Prevent Weight Loss?” Available at: http://www.builtlean.com/2012/11/26/alcohol-weight-loss/ [Accessed 24 February 2015]
- Hepatitis C Education & Prevention Society. (2015) “Stages of Liver Disease” Available at: http://hepcbc.ca/stages-of-liver-disease/ [Accessed 24 February 2015]
- MDidea. (2013) “Salvia miltiorrhiza and Salvia Species:identification,traditional use,application research of Radix Salvia miltiorrhiza and its useful fraction components.” Available at: http://www.mdidea.com/products/herbextract/danshen/data.html [Accessed 24 February 2015]
- Frazier, T.H., Stocker, A.M., Kershner, N.A., Marsano, L.S. and McClain, C.J. (2011) “Treatment of alcoholic liver disease.” Therapeutic Advances in Gastroenterology, 4(1):63-81.
- Botani, M. (2013) "Cirrhosis of the liver" Available at: https://www.youtube.com/watch?v=Sg7fEmnJ8lw [Accessed 02 March 2015]
