 Figure 1: Selection of anabolic steroids
Figure 1: Selection of anabolic steroids
Anabolic steroids are drugs that resemble androgenic hormones like testosterone. Steroids are used by athletes in order to facilitate an effort to gain muscle mass for increased muscular endurance and power. Steroids possess both androgenic and anabolic properties. Athletes rely more so on the anabolic properties which include the accelerated development of red blood cells, connective tissue and muscle. Since steroids are a substitution for the hormone
testosterone, prolonged use may cause a decrease in natural testosterone in the
body. As soon as steroids are administered, the body automatically recognises
the increase in testosterone levels and so it ceases natural testosterone
production.
When steroids were first developed, they were primarily used in the treatment of particular medical conditions. The anabolic effects of steroids usually involved stimulation of certain receptors in muscle cells which will then specifically target and activate genes. After administration of a steroid it will travel to the androgen receptors in muscle cells. The action of steroids begins when the exogenous hormone penetrates the membrane of the target cell and bind to the androgen receptor located in the cytoplasm. This activity causes the activation of hormone receptors which creates a messenger RNA (mRNA). The mRNA interacts with DNA in the cell and creates new proteins. The proteins travel throughout the body causing the anabolic responses and growth of muscle tissue. Anabolic steroids have both direct and indirect effects. The direct mechanism is a result of the effect the steroids have on the anabolic receptors which target gene transcription and regultate DNA accumulation. The indirect mechanism of the steroids are due to antiglucocorticoid action along with IGF-1 (insulin-like growth factor 1).
When steroids were first developed, they were primarily used in the treatment of particular medical conditions. The anabolic effects of steroids usually involved stimulation of certain receptors in muscle cells which will then specifically target and activate genes. After administration of a steroid it will travel to the androgen receptors in muscle cells. The action of steroids begins when the exogenous hormone penetrates the membrane of the target cell and bind to the androgen receptor located in the cytoplasm. This activity causes the activation of hormone receptors which creates a messenger RNA (mRNA). The mRNA interacts with DNA in the cell and creates new proteins. The proteins travel throughout the body causing the anabolic responses and growth of muscle tissue. Anabolic steroids have both direct and indirect effects. The direct mechanism is a result of the effect the steroids have on the anabolic receptors which target gene transcription and regultate DNA accumulation. The indirect mechanism of the steroids are due to antiglucocorticoid action along with IGF-1 (insulin-like growth factor 1).
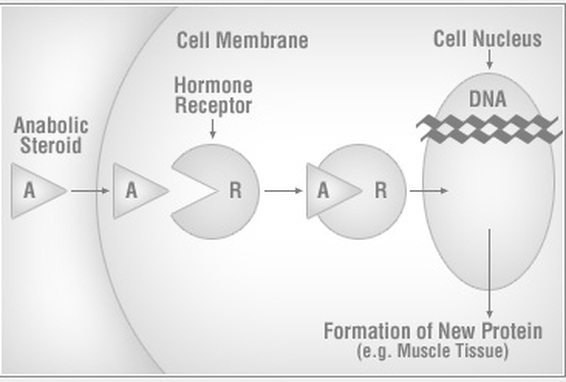
Figure 2: How anabolic steroids interact with receptors
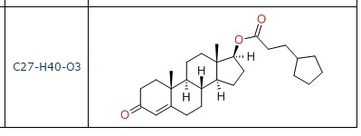 Figure 3: Structure of testosterone
Figure 3: Structure of testosterone
Steroid abuse can eventually lead to irreversible liver damage and cancers. Steroids consumed orally are harder for the liver to metabolize. This can cause difficulty for the liver in its ability to clear waste products. The use of anabolic steroids has been linked to many forms of liver toxicity such as hepatic tumours and chronic vascular injury to the liver. Many affects are associated with C-17 alkylated testosterones. Vascular changes within the liver have also been identified. Harmful changes in cholesterol levels have been noted in the case of long term steroid abuse. An increase in low-density lipoprotein (LDL) and decrease in high-density lipoprotein (HDL) causes a greater risk of heart attacks and strokes in patients. LDL is known as 'bad' cholesterol. It causes a hardening of the arteries and a build up of plaque. If some of this plaque were to break off, it may become lodged in smaller arteries and lead to a heart attack. HDL is thought to protect the cardiovascular system form heart disease but is less effective upon consumption of steroids.
Hepatocellular jaundice is another disease linked with anabolic steroid abuse. It is caused by hepatoxicity induced by steroids. Steroid-induced jaundice results in a yellowing of the sclera in the eye and skin. Cell necrosis affects the livers ability to metabolize and excrete bilirubin which causes a buildup of unconjugated bilirubin in the blood. Hepatic tumours are the most serious complication associated with steroid abuse. Prolonged use of between 5-15 years usually gives rise to tumours. The reason that bodybuilders suffer from the side effects of steroid abuse is due to the fact that they administer up to 40 times the recommended therapeutic dosage.
Peliosis hepatis is a syndrome in which blood filled sinusoids and cysts develop throughout the liver and the endothelial barrier becomes damaged. The liver becomes enlarged and fragile. The cysts are in danger of bursting which will lead to severe internal bleeding. Although this disease typically occurs in cancer patients, it is been known to be associated with anabolic steroid abuse with bodybuilders. The pathogenesis of peliosis is unknown but some potential causes include sinusoidal epithelial damage and increased sinusoidal pressure due to obstructed blood flow from the liver. Figures 4 & 5 seen below are examples of a patient with a healthy liver and of a patient who is suffering from Peliosis hepatis.
Hepatocellular jaundice is another disease linked with anabolic steroid abuse. It is caused by hepatoxicity induced by steroids. Steroid-induced jaundice results in a yellowing of the sclera in the eye and skin. Cell necrosis affects the livers ability to metabolize and excrete bilirubin which causes a buildup of unconjugated bilirubin in the blood. Hepatic tumours are the most serious complication associated with steroid abuse. Prolonged use of between 5-15 years usually gives rise to tumours. The reason that bodybuilders suffer from the side effects of steroid abuse is due to the fact that they administer up to 40 times the recommended therapeutic dosage.
Peliosis hepatis is a syndrome in which blood filled sinusoids and cysts develop throughout the liver and the endothelial barrier becomes damaged. The liver becomes enlarged and fragile. The cysts are in danger of bursting which will lead to severe internal bleeding. Although this disease typically occurs in cancer patients, it is been known to be associated with anabolic steroid abuse with bodybuilders. The pathogenesis of peliosis is unknown but some potential causes include sinusoidal epithelial damage and increased sinusoidal pressure due to obstructed blood flow from the liver. Figures 4 & 5 seen below are examples of a patient with a healthy liver and of a patient who is suffering from Peliosis hepatis.
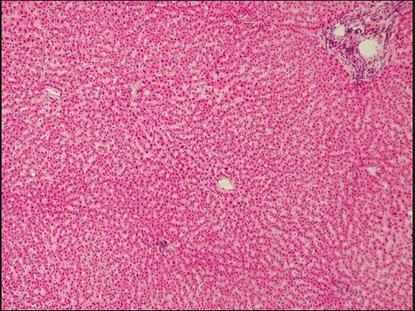
Figure 4: Image if a healthy liver tissue
|
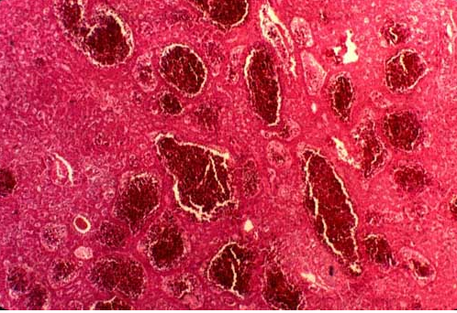
Figure 5: Peliosis hepatis in the liver. Blood filled cysts can be seen as the dark red circles. They are dangerous as they may burst and cause internal bleeding
|
- Sleisenger, M. 2006. “Sleisenger and Fordtran's Gastrointestinal and Liver Disease.” Philadelphia: W.B. Saunders Company
- Fahey, T.D. 1998. “Anabolic-androgenic steroids: Mechainsms of action and effect on performance.”
- Catlin, D.H. and Hatton, C.K. 1991. "Use and abuse of anabolic steroids and other drugs for athletic enhancement." Adv Int Med 36:399-424.
- Rogozkin, V. 1998. "Metabolism of Anabolic Androgenic Steroids." Leningrad: Nauka.
- Evans, N.A. 2004. "Current concepts in anabolic-androgenic steroids." Amer J Sports Med;32:534-42
- Ichijima, K., Kobashi, Y., Yamabe, H., Fujii, Y. and Inoue, Y. 1980. "Peliosis hepatis. An unusual case involving multiple organs". Acta Pathol. Jpn. 30 (1): 109–111
- Kicman, A.T. 2008. "Pharmacology of anabolic steroids." Br J Pharmacology. 154(3): 502-521.
- Images available at: -http://www.meddean.luc.edu/lumen/MedEd/orfpath/images/10-2-4.jpg - https://www.boundless.com/physiology/textbooks/boundless-anatomy-and-physiology- textbook/the-digestive-system-23/small-intestine-and-associated-structures-222/histology-of- liver-and-gallbladder-1088-1774/
- http://www.steroidabuse.com/how-anabolic-steroids-work.html
Page created by Alex Hickey
